Read the Reference Tables, Period analysis, Introduction and Chapter One below!
Also available on the kindle page.
Also available on the kindle page.
The legal/illegal boundary isn’t discovered in laboratories. It’s drawn in boardrooms and legislatures — and redrawn whenever the balance of profit shifts.
In 1898, Bayer sold heroin as a cough remedy. In 2023, the same company sells aspirin while fentanyl kills 100,000 Americans a year. The product changed. The mechanism didn’t.
Illicit Nation tracks 170 years of America’s dual drug economy — the pharmaceutical giants who manufacture dependency through legal channels, the enforcement agencies whose budgets grow regardless of outcomes, the banks that launder cartel billions and pay fines calibrated as cost-of-business, and the populations sorted by race and class into “patients” or “criminals” depending on which side of the boundary they stand.
This is not a policy book. This is muckraking.
From Mrs. Winslow’s Soothing Syrup killing infants with morphine to OxyContin’s FDA approval by a reviewer who later joined Purdue’s payroll. From the federal government poisoning industrial alcohol during Prohibition — killing an estimated 10,000 people to sustain a law it couldn’t otherwise enforce — to HSBC processing $881 million in cartel money and paying less than five weeks of revenue in penalties. From Nixon’s aide admitting that the War on Drugs was built to smash the anti-war movement and Black America to the same molecule carrying a 100:1 sentencing disparity depending on whether it was crack or powder cocaine.
The pattern is consistent, and it’s out in the open.
Across six parts — the unregulated market, classification, the pharmaceutical state, the war, the crisis, and the synthetic present — Illicit Nation shows how one system runs everything from street corners to telehealth pill mills, from heroin to ketamine clinics. It’s written for anyone who has ever been told the drug war is a tragic mistake, for families trying to understand what happened, and for workers who know they’re being chemically managed instead of materially supported.
Each chapter opens in scene — a Kensington street corner, an FDA approval meeting, a CIA safe house, a telehealth consult — then pulls back to show the machinery underneath. The writing is sharp, the evidence is blunt, and the argument builds into an indictment of a system that produces exactly what it is designed to produce.
The drug war isn’t failing. It’s working. Understanding how is the first step toward changing it.
Comprehensive Documentation:
Illicit Nation is built on hundreds of primary and secondary sources, including:
Congressional hearings and committee reports (Church Committee, Pike Committee, House Energy and Commerce Committee investigations)
Federal court documents, DEA filings, and FDA approval records
Declassified CIA archives (MK-Ultra, Contra-era operations)
SEC filings and corporate bankruptcy discovery (Purdue, Compass Pathways, HSBC deferred prosecution agreements)
Investigative journalism from the Washington Post, Los Angeles Times, Charleston Gazette-Mail, ProPublica and others
Foundational scholarship including Alfred McCoy’s The Politics of Heroin, David Courtwright’s Dark Paradise, Michelle Alexander’s The New Jim Crow, and Patrick Radden Keefe’s Empire of Pain
ARCOS distribution data, CDC mortality statistics, and U.S. Sentencing Commission reports
Every major claim is cited; the last 118 pages are the paper trail the system never meant you to read.

Parts I & II: The Unregulated Market + Classification - Above- Mrs Winslows Soothing Syrup (Baby Her oin) An Opium Den and an Opium "Institute"
Before the drug war, there was only commerce.
Mrs. Winslow's Soothing Syrup — morphine-laced, marketed to mothers — killed infants by the thousands. Bayer sold hero-in as a cough remedy through the same catalogues that offered aspirin. Cocaine appeared in toothache drops, patent tonics, and Coca-Cola. No prescriptions. No schedules. No crime. The substances that would define a century of prohibition circulated as freely as flour.
The Civil War created the first mass dependency. Military logistics distributed morphine at industrial scale; the hypodermic needle made administration efficient; "soldier's disease" named the outcome while obscuring its cause. The state produced the dependent population it would later pathologize. The for-profit sanitariums that emerged to treat these veterans — Keeley Institutes, private cures — were the first expression of a treatment industry that would extract profit from dependencies the system itself created.
Racial panic produced the first drug laws. San Francisco's 1875 opium den ordinance targeted Chinese users while white-owned pharmacies sold the same substance legally. The substance was the pretext; the target was the population. Immigration restriction and drug restriction shared infrastructure from the start.
Then the boundary was drawn.
The Harrison Narcotics Tax Act of 1914 began as a registration requirement and became, through enforcement, the foundation for American drug prohibition. Treasury agents prosecuted physicians for prescribing to dependent patients. The courts validated the transformation. What had been medicine became crime — but not for everyone. Chinese opium users faced prosecution while white pharmaceutical consumers faced nothing. The same molecule sat on both sides of the line; what differed was who consumed it.
Prohibition extended the logic and revealed its limits. The federal government poisoned industrial alcohol knowing bootleggers redistilled it for consumption — kill ing an estimated 10,000 Americans to maintain a law it couldn't otherwise enforce. Enforcement targeted immigrant and working-class communities while the wealthy drank legally through medical prescriptions and private clubs.
When Prohibition collapsed, the infrastructure didn't collapse with it. Harry Anslinger inherited the machinery. The Federal Bureau of Narcotics needed new enemies after alcohol was legal again. Anslinger invented the "marijuana menace" through fabricated stories — the "Gore Files" — of drug-induced violence by Black and Mexican users. The Marihuana Tax Act of 1937 proved that the classification system could survive its own failures by finding new targets.
Tobacco proved the corollary: powerful industries could escape classification regardless of harm. The most lethal recreational drug in history remained legal because the tobacco economy was embedded in Southern agriculture, federal tax revenue, and advertising-funded media. Classification was institutional, not pharmacological.
By 1945, the system was built: the legal/illegal boundary existed, racial sorting was constitutional, enforcement infrastructure was permanent, and the logic that would produce mass incarceration and pharmaceutical extraction was already operating. Everything that followed was shaped by what was constructed here.
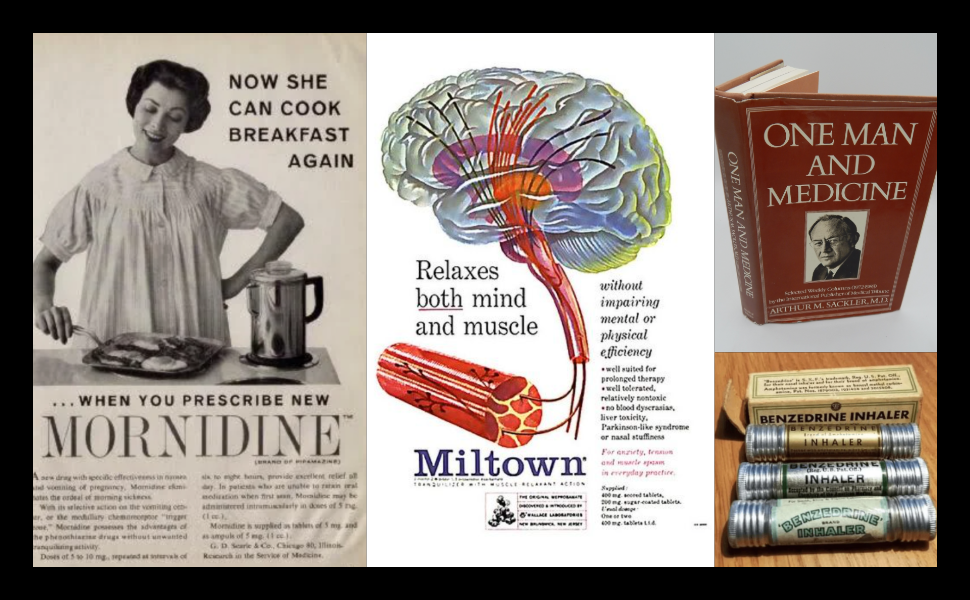
Part III: The Pharmaceutical State Above- Mornidine, Arthur Sacklers Tribuens Selected Works and Benzedrine- distributed to soldiers during WWII
The boundary had been drawn. Now it would be captured.
World War II changed everything. The military distributed amphetamines to soldiers for combat readiness — millions of doses, industrial scale, government logistics. When the war ended, the pharmaceutical industry recognized what the state had demonstrated: psychoactive substances could be distributed at mass scale through official channels. The legal side of the boundary was territory to be occupied.
The sedative pipeline opened: bromides to barbiturates to Miltown to Valium, each generation marketed as safer than its predecessor, each producing dependencies that fueled demand for the next. Miltown became America's first mass-market tranquilizer. Valium became the most prescribed drug in the country from 1968 to 1982. Women were prescribed sedatives at twice the rate of men — female distress pathologized, chemically managed, profit extracted from the prescription pad.
The stimulant pipeline ran parallel: Benzedrine inhalers sold over the counter, diet pills prescribed to millions of women, amphetamines distributed to truck drivers and factory workers for productivity. The same molecule sorted by class — therapeutic for middle-class dieters, criminal for working-class speed users. The boundary ran through the pharmacy counter.
Arthur Sackler invented the playbook. He owned Medical Tribune (physician publication) and IMS Health (prescription tracking data) while running the advertising agency that promoted Valium. Funded research, branded journal advertising, sales representatives detailing physicians — the techniques his family would later use to sell OxyContin. The playbook worked then. It worked again.
The CIA ran MK-Ultra. The same government criminalizing LSD for civilians administered LSD to unwitting American citizens — in universities, in prisons, in Operation Midnight Climax safe houses where prosti tutes dosed customers for observation. Sidney Gottlieb destroyed most of the records. What survived proved that the state's relationship to dru gs was never prohibitionist. It was instrumental.
The Hero-in Highway opened: CIA-supported anti-communist forces in Southeast Asia controlled opium production. Air America flights moved product. French Connection processing in Marseille converted opium to hero-in for American markets. The geopolitical model required drug-producing allies; the domestic system criminalized the supply those allies produced.
The Controlled Substances Act of 1970 locked the system into place. Schedule I — "no accepted medical use" — created permanent prohibition for substances the government itself had tested as weapons. The counterculture provided political justification. The pharmaceutical industry shaped the architecture. The Attorney General gained authority to schedule substances without congressional approval.
The contradiction persists: the same molecule is medicine on one side of the boundary and crime on the other. The difference is who controls distribution.
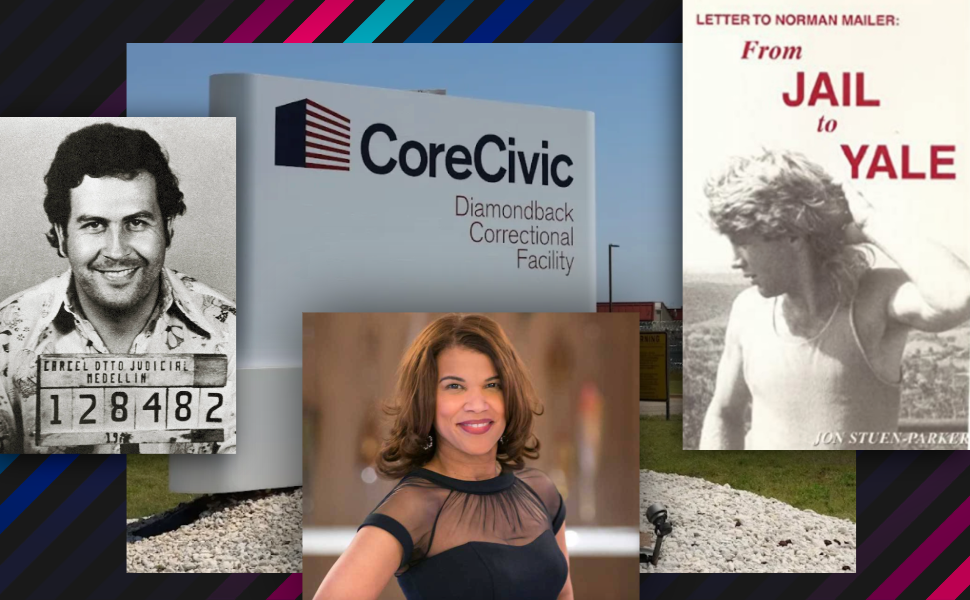
Part IV: The War Above- Pablo Escobar , Coreciviv Private Prison Facility, Kemba Smith and John Stuen Parker
"We knew we couldn't make it illegal to be either against the war or Black, but by getting the public to associate the hippies with marijuana and Blacks with hero-in, and then criminalizing both heavily, we could disrupt those communities."
John Ehrlichman, Nixon's domestic policy advisor, confessed the War on Dru gs' purpose decades after its launch. The confession confirmed what the evidence had always shown: drug classification was political warfare dressed as public health.
The DEA was created in 1973. Its budget has never decreased — not when drug use declined, not when strategies failed, not when the bodies accumulated. Asset forfeiture allowed enforcement to fund itself through property seizures, no conviction required. Equitable sharing let local police bypass state restrictions by partnering with federal agencies. Private prisons — CoreCivic, GEO Group — created corporate constituencies for incarceration, with contracts guaranteeing minimum occupancy. The war became an industry. Continued conflict, not victory, was the sustainable business model.
Mandatory minimums eliminated judicial discretion. Plea bargains processed 97% of federal drug cases without trial. The coercion was structural: defendants accepted deals because trial risked catastrophic sentences. Surveillance infrastructure — drug testing, probation monitoring, PDMP databases — extended carceral control beyond prison walls. The system didn't just incarcerate. It managed populations.
The crack/powder disparity made the racial mechanism statutory. Same molecule — cocaine. 100:1 punishment ratio based on form. Crack, prevalent in Black urban communities, triggered mandatory minimums at 5 grams. Powder, prevalent in white professional circles, required 500 grams for the same sentence. The pharmacology was identical. The populations were not. Kemba Smith — first-time offender, 24.5 years.
The Medellín cartel demonstrated what prohibition produces: revenue exceeding Colombia's GDP, violence that destabilized a nation, organizational infrastructure that survived the death of any individual leader. When Escobar fell, Cali expanded. When Cali fell, Mexican organizations took over. The supply chain adapted. Prohibition created the superprofits; the superprofits created the power.
The Contra-cocaine connection proved imperial complicity. CIA-backed Nicaraguan Contra forces, cut off from congressional funding, moved cocaine through Los Angeles — through Danilo Blandón, through Ricky Ross, into communities the DEA would then devastate. Gary Webb documented it. The major newspapers destroyed him. The CIA Inspector General confirmed it. Nothing changed.
Meth revealed class sorting in real time: pharmacologically near-identical to Adderall, but meth users faced prosecution while Adderall users got prescriptions. Rural and working-class users criminalized; professional-class users medicalized. Same molecule, different bodies, different outcomes.
Harm reduction was criminalized. Jon Parker was arrested for distributing clean needles. The federal funding ban on needle exchange persisted for 27 years despite overwhelming evidence of effectiveness. HIV spread through populations that enforcement had concentrated in the shadows. The system preferred infection to acknowledging that prohibition produced harm.
By 1996, the machinery was complete: enforcement economics, mass incarceration, imperial complicity, and the racialized sorting that processed millions of bodies through courts and prisons. The war produced exactly what it was designed to produce.
Parts V & VI: The Crisis - Above- Oxycontin, and the propaganda Purdue put out. Paxil, an "antidepressant" that lead to inumerable suicides.
The boundary dissolved at the top — and then it fragmented entirely.
The Pharmaceutical Crisis (Part V): OxyContin launched in 1996 with FDA label language drafted by Purdue and approved by a reviewer who later joined Purdue's payroll. The marketing followed Arthur Sackler's playbook: funded medical education, sales representatives detailing physicians, pain reframed as undertreated epidemic. Result: mass prescription, mass dependency, half a million dead.
The distribution system was complicit. McKesson shipped nine million pills to a pharmacy in Kermit, West Virginia — population 382. HSBC laundered $881 million in cartel money and paid less than five weeks of revenue in fines. The boundary that imprisoned street dealers for decades processed corporate perpetrators in months.
But opioids weren't alone. The SSRI pipeline ran parallel — the serotonin hypothesis marketed as settled science, clinical trial data suppressed, dependency rebranded as "discontinuation syndrome." GSK's Study 329 showed Paxil ineffective and dangerous for adolescents; the ghostwritten published version claimed the opposite. ADHD diagnosis expanded from 3% to 11% of children, creating a school-to-prescription pipeline that sorted professional-class kids toward Adderall while working-class adults faced meth prosecution for the same molecule. The for-profit rehab industry extracted from dependencies the system created — 28-day programs based on insurance limits, not clinical evidence, with treatment courts creating captive markets.
The Synthesis (Part VI): When prescription opioids tightened, the market shifted to hero-in, then to fentanyl — synthetic, potent, with global supply chains the classification system was never designed to govern. Overdose deaths hit 100,000 annually and stayed there.
Cannabis legalization proved the boundary could move without justice following. Corporations backed by private equity dominate the legal industry while 40,000 remain incarcerated for the same substance. Social equity provisions are underfunded window-dressing. The dispensary and the prisoner exist simultaneously.
Platform technology enabled prescription at industrial scale. Cerebral and Done — telehealth startups backed by hundreds of millions in venture capital — prescribed controlled substances through ten-minute video consultations, replicating pill mill economics digitally. The DEA investigated; the model had already scaled.
Grey markets proliferate where classification fails: kratom in gas stations, delta-8 THC exploiting Farm Bill loopholes, research chemicals through the mail, nootropics in Silicon Valley offices. The professional class self-medicates with impunity while the working class faces prosecution for pharmacologically comparable substances.
And now the cycle completes: psychedelics, criminalized after MK-Ultra leaked into the counterculture, are being medicalized through venture capital. Compass Pathways went public at over $1 billion valuation. MAPS coordinates FDA trials. The same substances the CIA tested on unwitting citizens are becoming pharmaceutical commodities — with patents on therapy protocols and pric ing models that will determine who gets access.
The contradiction doesn't resolve. It reproduces at higher complexity. The boundary fragments, multiplies, and the extraction continues regardless.
Introduction: The Same Molecule
The corner of Kensington and Allegheny avenues in Philadelphia sits on what used to be the industrial floor of the richest nation on earth. The textile mills are gone. The carpet factories are gone. The hat manufacturers, the metalworks, the tanneries that once employed the neighbourhood’s German and Irish and Polish residents — all gone, shipped out or shut down across four decades of deindustrialisation that nobody in power calls by its proper name.¹ What replaced them is the largest open-air drug market on the eastern seaboard of the United States.
Stand on that corner long enough and you will see every function of the American drug economy operating at once. Not sequentially, not in separate neighbourhoods, not divided by some clean analytical line — simultaneously, through the same bodies, on the same block.
Start with labour. The men and women buying fentanyl at Kensington and Allegheny are not, for the most part, recreational users who stumbled into dependency through poor choices. A significant proportion are injured workers — former warehouse employees, construction labourers, service workers whose bodies broke under conditions their employers refused to make safe.² They got prescriptions. The prescriptions ran out, or their insurance lapsed, or a new guideline tightened the supply. The pain didn’t stop. The street supplied what the pharmacy wouldn’t. This is not a story about personal weakness. This is chemical management of a labour force — the same function opium served for injured Civil War veterans in the 1860s, the same function Pervitin served for German factory workers in the 1940s, the same function Adderall serves for gig workers today. The substance changes. The function doesn’t.
Now look at the economy. Kensington’s unemployment rate has hovered around three times the city average for decades.³ The drug market is not a deviation from the local economy — it is the local economy. It employs runners, lookouts, packagers, distributors, drivers. It circulates cash through bodegas, laundromats, prepaid phone vendors. In a neighbourhood where legitimate capital withdrew, the drug economy absorbed the surplus population that deindustrialisation produced. This is not a failure of capitalism. This is capitalism working exactly as designed: when profitable employment disappears, other markets fill the vacuum, and those markets will be whatever the conditions of profitability allow.
Now look at who gets arrested. Philadelphia police make drug arrests at Kensington and Allegheny on a regular rotation. The people arrested are overwhelmingly Black and Latino, in a neighbourhood that was, until the 1990s, predominantly white working class.⁴ Three blocks east, a pharmacy dispenses buprenorphine by prescription. The molecular difference between the fentanyl sold on the corner and the buprenorphine dispensed at the pharmacy is real but pharmacologically minor. Both act on the same opioid receptor system. Both produce dependency. Both relieve pain. The difference that matters is not chemical. It is classificatory. One substance sits on Schedule II of the Controlled Substances Act; for years, prescribing the other required a special DEA “X-waiver” — a bureaucratic choke point that kept supply scarce even as overdose deaths climbed. Both are opioids acting on the same receptor system, but one is packaged as treatment and the other as a crime. Which one you encounter depends on your insurance status, your zip code, and the colour of your skin. The boundary between “licit” and “illicit” is not drawn by pharmacology. It is drawn by political economy. And the people who drew it profited from both sides.
Now follow the supply chain backwards. The fentanyl sold at Kensington and Allegheny was, in most cases, synthesised in clandestine laboratories in the Mexican states of Sinaloa or Jalisco, using chemical precursors shipped from Chinese manufacturers, ordered through encrypted messaging platforms, paid for in cryptocurrency, and delivered by commercial freight through ports that process millions of containers per year.⁵ The supply chain that delivers fentanyl to a Philadelphia street corner is a global logistics operation — as rationalised, as cost-efficient, and as ruthlessly optimised as any supply chain operated by Amazon or Walmart. The difference is that this supply chain exists because the legal supply chain was constricted. Every kilo of fentanyl sold at Kensington represents a market that pharmaceutical companies created, that enforcement agencies made illegal, and that trafficking organisations then serviced at higher margins with lower quality control. The imperial circuit — foreign production, domestic consumption, profit extraction at every node — is the same circuit that moved Turkish opium through Corsican labs to American cities in the 1960s, the same circuit that moved Colombian cocaine through Nicaraguan Contras to Los Angeles in the 1980s. The geography shifts. The structure persists.
Four functions, one corner. It manages labour, soaks up the surplus, sorts people, and feeds an empire. That isn’t a malfunction. That’s the machine doing exactly what it was built to do — every mechanism from 170 years of American drug policy running at once through the same patch of pavement. This is what the book you are holding is about.
It was not always this way. Or rather: the mechanism was always this way, but the machinery around it was not.
In 1898, the Bayer pharmaceutical company of Elberfeld, Germany, began marketing a new product. The company’s chemists had synthesised diacetylmorphine — a derivative of morphine — and the commercial department branded it with a name designed to evoke the German word heroisch, meaning heroic, for the way it made patients feel. They called it Heroin.⁶
Bayer sold Heroin as a cough suppressant and a “non-addictive” substitute for morphine. The advertisements ran in medical journals and popular publications alike. You could buy it at the drugstore without a prescription. Bayer’s marketing literature recommended it for children.⁷ There was no legal boundary between Heroin and any other pharmaceutical product, because no such boundary existed. The same company sold aspirin. The distinction between the two products was therapeutic, not legal. Nobody went to prison for buying Bayer’s Heroin, and nobody went to prison for selling it. The molecular compound that would later anchor the most punitive enforcement regime in American history was, in 1898, a consumer product with a cheerful brand name and a targeted advertising campaign.
This is not an odd historical footnote. It’s the cleanest starting point for what this book argues: “illicit” is not a property of substances. It is a classification produced by material interests — by pharmaceutical companies seeking market share, by enforcement agencies seeking budgets, by politicians seeking elections, by insurers seeking profit, by states seeking population control. The same molecule — the exact same molecule — that Bayer marketed for children’s coughs in 1898 would, within two decades, become the basis for federal criminal prosecution. What changed was not the chemistry. What changed was who profited from classification, and who paid for it.
Between Bayer’s advertisement and Kensington’s street corner, 130 years elapsed. In that time, the United States built the most elaborate drug classification system in the world. It created an entire federal enforcement agency — the Drug Enforcement Administration — whose budget has never shrunk in any year since its creation.⁸ It incarcerated more of its own citizens for drug offences than any other nation in human history.⁹ It spent over a trillion dollars on drug enforcement.¹⁰ It launched covert operations on four continents to control drug supply chains while simultaneously profiting from them. It allowed pharmaceutical companies to produce mass opioid dependency through legal prescriptions while imprisoning the people who used the same molecules obtained through illegal channels. And at the end of those 130 years, dependency rates are higher, drug-related mortality is higher, enforcement spending is higher, and incarceration numbers are higher than at any point in the nation’s history.¹¹
This is not a story of policy failure. Policy failure implies that the policy was trying to do what it said it was trying to do. The drug policy of the United States has never been primarily about reducing drug use. It has been about managing populations, extracting profit, and maintaining a classification boundary that serves the interests of capital. By that measure — the measure of what the system actually does rather than what it claims to do — American drug policy has been one of the most successful domestic programmes ever implemented.
This book is not a pharmacology textbook. You’ll only see brain chemistry when it’s needed to show how companies hid behind it. It isn’t a recovery memoir either. There’s no “my journey” chapter, because turning dependency into a personal quest is one of the ways the system ducks responsibility. It isn’t a policy white paper with a ten-point plan at the back. The claim here is simple: you don’t fix this by tightening a few screws; you change the machine. And it definitely isn’t a “both sides” account. There aren’t two equally valid views of a programme that produces 110,000 overdose deaths a year.¹²
The book builds on three essential predecessors, and departs from each.
Alfred McCoy’s The Politics of Heroin in Southeast Asia, first published in 1972, demonstrated that the Central Intelligence Agency’s Cold War alliances with opium-producing warlords in Southeast Asia directly facilitated the heroin supply that flooded American cities in the 1960s and 1970s.¹³ McCoy got the imperial supply chain right — the connection between geopolitics abroad and drug markets at home. But McCoy’s analysis stops at the water’s edge. He traces how heroin gets to the United States. He does not trace what happens after it arrives: who profits from enforcement, who profits from treatment, how the classification boundary is maintained domestically, how the pharmaceutical industry operates as the legal mirror of the trafficking organisations he documents.
David Courtwright’s Dark Paradise: A History of Opiate Addiction in America, published in 1982 and revised in 2001, provides the most comprehensive historical account of opiate dependency in the United States from the Civil War to the late twentieth century.¹⁴ Courtwright gets the history right — the patent medicines, the physician addicts, the Harrison Act, the demographic shifts. But Courtwright frames his account as medical and social history. The organising force in Dark Paradise is the substance itself and the medical profession’s evolving relationship to it. Capital — the profit motive that drives production, classification, and enforcement — remains in the background. The system that Courtwright describes so carefully is there in every chapter; it just never gets called by its real name.
Gary Webb’s “Dark Alliance” series, published in the San Jose Mercury News in 1996 and expanded into a book in 1998, documented the connection between the CIA-backed Nicaraguan Contras and the crack cocaine epidemic in Los Angeles.¹⁵ Webb demonstrated that the United States government’s covert foreign policy directly supplied the raw material for the most devastating drug crisis in American urban history — and that enforcement agencies knew and did nothing. Webb got the conspiracy right, and it was a conspiracy: a documented, traceable chain of supply from Contra operatives through Danilo Blandón and “Freeway” Ricky Ross to the streets of South Central Los Angeles. For his trouble, Webb was professionally destroyed. The Los Angeles Times assigned seventeen reporters to discredit his series. The Mercury News retracted its support. Webb was demoted, resigned, and died of suicide in 2004.¹⁶ What happened to Gary Webb is itself evidence for the argument of this book: the system does not merely operate through policy. It operates through the destruction of the people who reveal it.
None of these works tries to follow the whole circuit end to end. Illicit Nation does, and it treats it as one system. Production, classification, enforcement, extraction, treatment, and back again. Not as separate stories, not as parallel histories, but as an integrated structure operating across 170 years of American capitalism. The pharmaceutical company that markets the drug, the enforcement agency that classifies it, the regulator that approves it, the insurer that gatekeeps it, the trafficker that supplies the illegal alternative, the treatment industry that profits from the dependency, the prison system that warehouses the bodies — these are not separate actors pursuing separate interests. They are positions inside a single machine, and the machine produces its outcomes not despite its contradictions but through them. The same system that creates dependency criminalises it. The same system that manufactures the legal supply creates the conditions for the illegal supply. The same system that profits from selling the drug profits from punishing its use.
The working method of this book is straightforward: follow the money, follow the law, follow the bodies. When there is a contradiction — a law that claims one thing and clearly does another, a company that markets safety and produces mass harm, an agency that says “treatment” and funds cages — that contradiction is treated as a clue, not a mistake. Each chapter asks the same questions: who pays, who profits, who gets managed, who disappears from the story? Over time, the answers stop looking like isolated scandals and start to look like design.
This book covers six stages, each defined by the form the central contradiction takes.
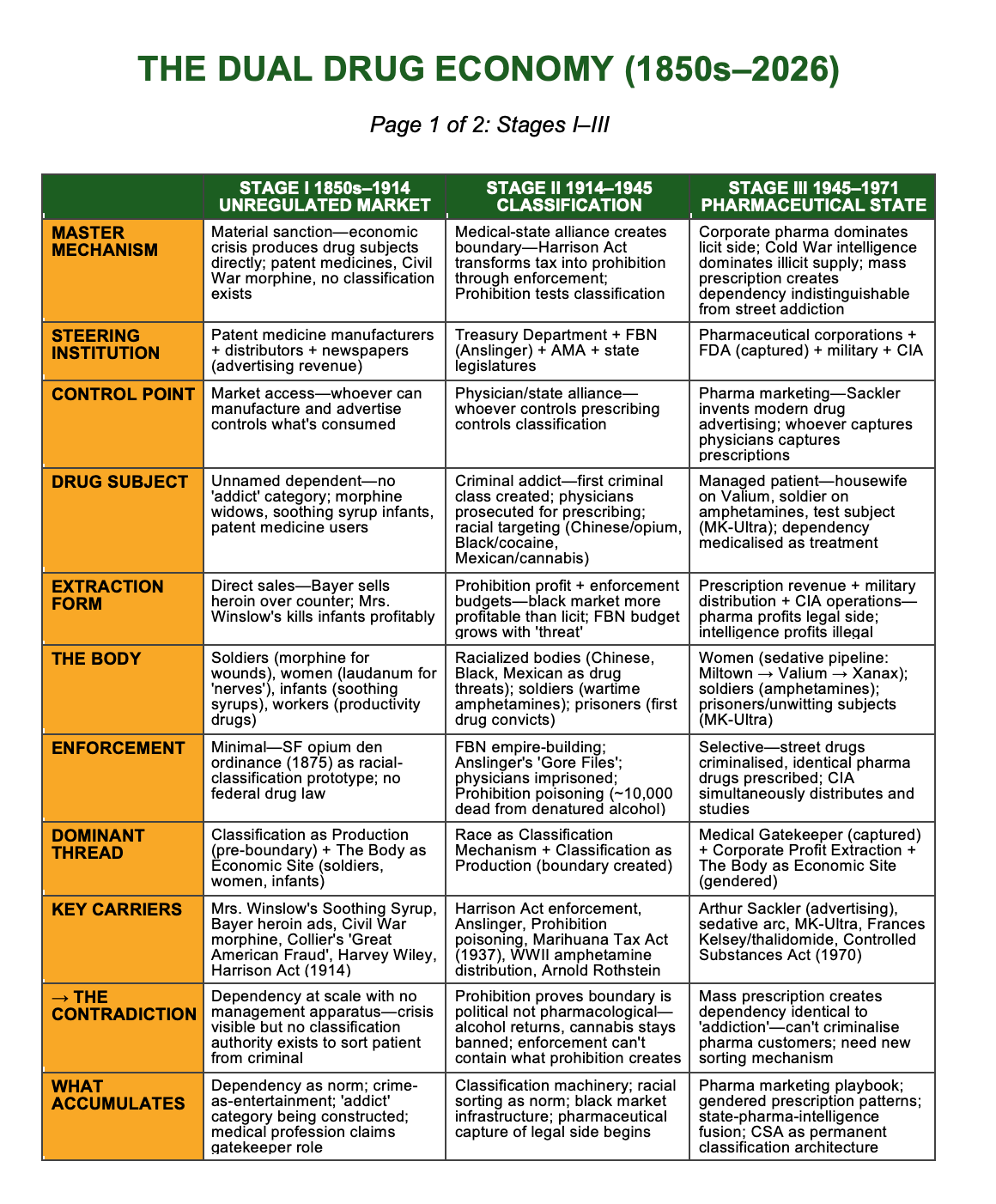
The first stage, from the 1850s to 1914, is the unregulated market. Patent medicines sold freely in grocery stores and through mail-order catalogues, containing opium, morphine, cocaine, and heroin in doses that killed infants and produced dependency in millions of adults who never knew what they were swallowing. The United States Army distributed morphine to wounded soldiers by the trainload during the Civil War, creating a generation of dependent veterans whose condition was named “the army disease” — as though the dependency were something the soldiers had contracted rather than something the state had administered.¹⁷ No legal/illegal boundary existed. That boundary had to be invented, and it was invented to serve specific interests.
The second stage, from 1914 to 1945, is the creation of that boundary. The Harrison Narcotics Tax Act of 1914 — framed as a tax measure, enforced as prohibition — established the legal architecture that would grow into the Controlled Substances Act. Prohibition tested the boundary and demonstrated that criminalisation creates its own economy. Harry Anslinger, appointed head of the Federal Bureau of Narcotics in 1930, built his agency’s budget and his personal career on the racial weaponisation of drug classification: marijuana associated with Mexican labourers, cocaine with Black men, opium with Chinese immigrants.¹⁸ The classifications were not scientific. They were economic and racial — tools for managing populations that threatened the labour hierarchy.
The third stage, from 1945 to 1971, is the pharmaceutical capture of the legal side. The tranquilliser boom put millions of American women on Miltown and then Valium — chemical management of the gendered labour force, sold as medicine for “anxiety.” The U.S. military distributed amphetamines to soldiers in Korea and Vietnam. The CIA dosed unwitting American citizens with LSD under MK-Ultra while the same agency facilitated heroin trafficking by its allies in Southeast Asia.¹⁹ The system was using on its own population the very substances it was criminalising its own population for using.
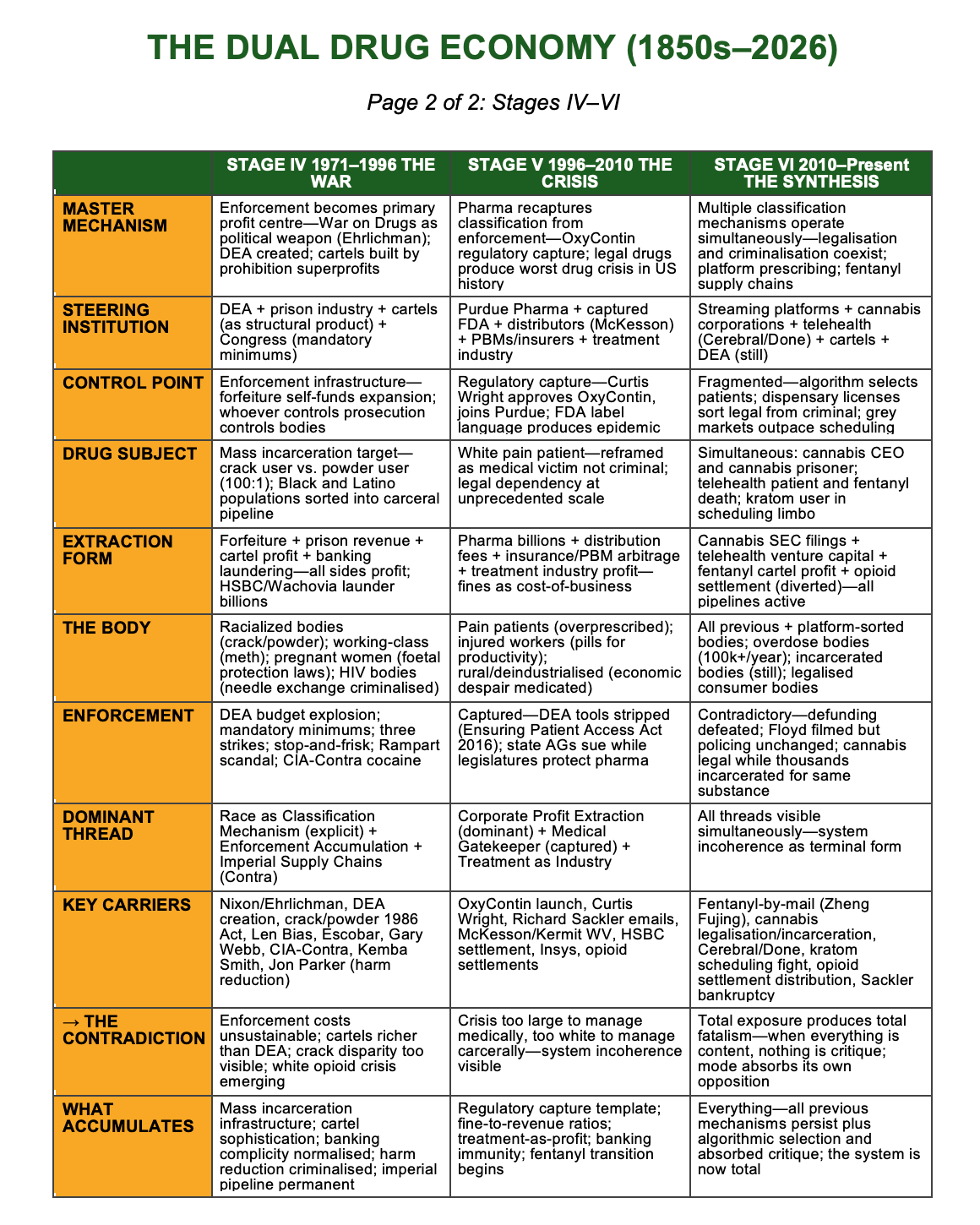
The fourth stage, from 1971 to 1996, is the War on Drugs. Nixon’s domestic policy adviser John Ehrlichman would later confess that the war was designed to target Black communities and the antiwar left — that drug classification was a political weapon.²⁰ The DEA was created. Asset forfeiture turned enforcement into a profit centre. The Anti-Drug Abuse Act of 1986 imposed a 100:1 sentencing disparity between crack and powder cocaine — the same molecule, different sentencing based on the race and class of the user population.²¹ And while the War on Drugs was being waged at home, the CIA was facilitating cocaine trafficking through Contra networks that pumped cheap crack into the cities being most heavily policed.
The fifth stage, from 1996 to 2010, is the opioid crisis. Purdue Pharma’s OxyContin, approved by the FDA in 1995, was marketed on the fraudulent claim that its extended-release formulation made it less addictive. The FDA medical reviewer who approved OxyContin, Curtis Wright, left the agency and took a job at Purdue within two years.²² McKesson and AmerisourceBergen shipped millions of pills to pharmacies in towns too small to consume them — the data visible in real time through the DEA’s own ARCOS tracking system, and ignored.²³ HSBC laundered $881 million for Mexican and Colombian cartels and paid a $1.9 billion fine — less than five weeks of the bank’s annual profit — with no criminal prosecution.²⁴ The boundary dissolved at the institutional level. At the street level, it hardened.
The sixth stage, from 2010 to the present, is the synthesis — fentanyl supply chains operating with the efficiency of global logistics, cannabis legalisation captured by corporate capital while tens of thousands remain incarcerated for cannabis offences, platform prescribing through telehealth apps that reproduce the pill mill model digitally, grey markets that blur every line the classification system drew.²⁵ The contradiction is not resolving. It is reproducing at higher complexity.
Across these stages, the core contradiction stays the same; it just keeps changing shape. The system needs both the substance and the prohibition. It needs both the legal pill and the illegal powder. It needs both the pharmaceutical pipeline and the prison one. What changes from stage to stage is who controls each side and how the boundary between them is drawn.
Eight threads run through all six stages.
Classification as production: the legal/illegal line is not discovered in a lab; it is drawn and redrawn as interests shift. Corporate and financial actors extract profit on both sides of that line — from the pills and from the “compliance” work once those pills go off-book. Bodies — soldiers, workers, women, children — are chemically managed so they can be sent back to work or kept out of sight. Race keeps turning up as the sorting tool for who gets a clinic and who gets a cell. The drug economy is never just “domestic”: imperial supply chains feed American markets while enforcement reaches into the same countries that were encouraged to produce. Labour is managed chemically, from Civil War morphine through factory-floor amphetamines to modern stimulant prescriptions. Treatment itself becomes an industry, with profit extracted from chronic relapse. And whoever controls access — doctors, regulators, insurers, platforms — controls the boundary.
These threads do not start and stop. They accumulate.²⁶
And this is the most important structural claim the book makes: the system is sedimentary. Every stage adds new machinery. Nothing gets dismantled. The Harrison Act’s enforcement logic persists inside the Controlled Substances Act. Anslinger’s racial classification persists inside the DEA’s arrest patterns. The pharmaceutical industry’s capture of medical authority persists inside the FDA’s approval process. The War on Drugs’ self-funding enforcement model persists inside asset forfeiture law. OxyContin’s prescription-to-street pipeline persists inside the fentanyl crisis. Each new stage builds on top of what came before. Each new “reform” is another layer of plaster over the same infected bone. The DEA’s budget has grown every single year since the agency’s creation in 1973 — through Republican administrations and Democratic ones, through declared drug wars and declared truces, through crises that were supposed to end and crises that were supposed to be solved.²⁷ The system does not reform. It accumulates.
You can see every layer on that corner in Kensington. The Harrison Act logic that made opioid possession a federal crime. Anslinger’s racial classification, still visible in who gets arrested and who gets treatment. The pharmaceutical marketing that produced the dependency in the first place. The War on Drugs infrastructure that processes the arrests. The OxyContin pipeline that moved patients from prescription to street supply. The fentanyl supply chain that replaced the old heroin networks with something cheaper, stronger, and more lethal. None of these layers has been removed. They are all still operating, simultaneously, through the same bodies, on the same block.
A hundred and thirty years separate Bayer’s heroin advertisement from Kensington’s fentanyl market. In that time, the United States created, expanded, and weaponised a drug classification system that has incarcerated millions, enriched corporations, funded covert wars, managed labour forces, sorted populations by race and class, and produced more dependency and more death in every decade than the one before. The system was never broken. It was built this way. What follows is the record of how it was built, who built it, who profited, and who paid.
Before the boundary existed, there was only trade.
Mrs. Winslow’s Soothing Syrup packed morphine and was sold to mothers for teething infants. Bayer sold heroin as a cough remedy in the same catalogues that offered aspirin. Cocaine turned up in toothache drops, patent tonics, and Coca-Cola. The very substances that would later anchor a “drug war” simply moved through pharmacies, general stores, and mail-order houses like anything else — no prescriptions, no schedules, no legal line between the customer buying laudanum and the one buying flour.
This wasn’t chaos. It was capitalism without a classification system. Dependencies existed but had no structural name: “soldier’s disease” for veterans, “nerves” for middle-class women, “weakness” or “degeneracy” for the poor. The machinery that would later sort people into legal and illegal, patient and criminal, had not yet been built. The state hadn’t yet claimed the power to decide which substances could circulate and which could not, which forms of dependency counted as medicine and which as crime.
Part I follows the build-up to that moment: the conditions that made a boundary useful and the interests that wanted to draw it. Patent-medicine death rates created pressure for “reform” — infants killed by morphine syrups advertised as soothing produced outrage that moral crusaders could tap. Civil War logistics produced the first mass iatrogenic dependency — the state itself saturating soldiers with opiates, then pathologising the result. Anti-Chinese panic over opium dens produced the first local drug ordinances — a test run for using “drug control” as labour and racial control. Medical professionals pushed for gatekeeping; the AMA wanted power over prescribing and a monopoly position that patent-medicine traders had cut around.
By 1914, everything was on the table: high death rates, imperial manoeuvring, professional lobbying, racial fear. All that was missing was a law.
The chapters that follow move from open commerce to the edge of regulation — from substances flowing wherever there was money, to the moment when the state decided some flows needed to be fenced. The core contradiction is already visible: the same interests that profit from distribution will profit from restriction. The same people harmed when access is unregulated will be hammered again when access is criminalised. The boundary that Part II builds will not solve that contradiction. It will lock it into law.
In 1884, a coroner in the English town of Salford recorded the death of a five-week-old infant. The cause of death was morphine poisoning. The source was a product called Mrs. Winslow’s Soothing Syrup, purchased over the counter by the child’s mother for sixpence, administered as directed on the label. The label said the syrup would quiet teething pain and help the baby sleep. The label did not say the syrup contained morphine sulphate.¹
The woman whose name was on the bottle, Mrs. Charlotte N. Winslow, had been a nurse. Her son-in-law, Jeremiah Curtis, and his business partner, Benjamin A. Perkins, took the family recipe, bottled it in Bangor, Maine, and built a transatlantic brand.² “Mrs. Winslow” herself turned into a logo: a grandmotherly silhouette and a promise that this was a kindly domestic remedy, not a dangerous drug. The syrup was advertised as “likely to soothe any human or animal.” It did exactly that, because every fluid ounce contained dozens of milligrams of morphine along with aromatics and alkalis. The dosage was high enough that a few spoonfuls could stop a baby crying, stop their breathing, or both.
The Salford coroner’s report was not unusual. It was one of dozens recorded across England and the United States in the 1880s and 1890s — dead infants, all dosed with commercially available preparations containing opium, morphine, or both, all purchased legally, all administered by parents who had no way to know what was in the bottle. The British Medical Journal published warnings. The American Medical Association published warnings. Mrs. Winslow’s Soothing Syrup continued to sell. It had been on the market since the 1840s and would remain available, in various formulations, into the early twentieth century.² Millions of bottles were sold annually across two continents.³ The product was not hidden, not illegal, not difficult to obtain. It sat on the same shelf as cough drops and tooth powder.
Decades later, in 1911, the American Medical Association rounded up infant “remedies” like Mrs. Winslow’s in a book bluntly titled Nostrums and Quackery. The chapter heading that covered Soothing Syrup and its competitors was “Baby Killers.” The AMA laid out the morphine content, the casualty trail, and the lies on the label in plain English.²² By then, Curtis & Perkins had already spent years deflecting criticism, tweaking formulas just enough to stay ahead of local prosecutions, and leaning on their advertising allies. Even after the AMA publicly branded their product a child-killer, Soothing Syrup did not vanish overnight. In some markets it lingered into the 1920s. A remedy that coroners and doctors knew was killing children remained legal and widely promoted for roughly half a century after those deaths began to be recorded.
This is where the story of “illicit” begins — not with a crime, not with a boundary, not with enforcement, but with a dead baby and a legal product and a market that had no reason to stop selling either.
The patent medicine economy of the late nineteenth century was not a marginal curiosity. It was one of the largest consumer industries in the United States. By the 1890s, Americans were spending approximately $75 million per year on patent medicines — a figure that would exceed $3.5 billion in today’s dollars.⁴ The products were sold in drugstores, grocery stores, and general merchants. They were ordered through the Sears, Roebuck catalogue. They were advertised in every major newspaper in the country and in thousands of minor ones.
They carried names designed to sound scientific — Dr. James’ Soothing Syrup Cordial, Godfrey’s Cordial, Ayer’s Cherry Pectoral, Hamlin’s Wizard Oil — and names designed to sound wholesome and domestic, like Lydia E. Pinkham’s Vegetable Compound, fronted by a matronly portrait and pitched as a tonic for “female complaints.” They contained ingredients designed to make you feel better immediately: opium, morphine, heroin, cocaine, chloroform, alcohol, and cannabis, in combinations and concentrations that varied by batch and were disclosed to nobody.⁵ A bottle of Pinkham’s Compound might be nearly 20 percent alcohol. A bottle of Hostetter’s Bitters was closer to a strong wine than a medicine. The label language was about nerves, strength, and purity; the contents were about sedation.
Behind the labels sat families and firms that would become fixtures of American business history. The Pinkhams, the Perunas, the men behind Piso’s Cure and Hood’s Sarsaparilla built fortunes on “cures” that were mostly ethanol and opiates. They advertised themselves as pillars of the community and benefactors of the sick. Their companies incorporated, passed shares to heirs, donated to churches and civic projects, and quietly fought every attempt to make them say what was in the bottle.
The industry operated on a simple principle. You sold a product that contained a dependency-producing substance. The consumer didn’t know the substance was present. They knew only that the product worked — their cough stopped, their pain eased, their baby slept. When the product wore off, the symptoms returned, often worse than before, because the body had begun to adjust to the substance it didn’t know it was receiving. The consumer bought more. The manufacturer shipped more. The cycle was self-reinforcing and enormously profitable, and it required no conspiracy, no cartel, no enforcement regime — just an unregulated market and an unlabelled bottle.
This was dependency production at industrial scale, and it predated every institution that would later claim authority over the problem. The DEA did not exist. The FDA did not exist. The Controlled Substances Act did not exist. The Harrison Narcotics Tax Act did not exist. No legal boundary separated the morphine in Mrs. Winslow’s Soothing Syrup from the morphine a physician injected into a patient’s arm. Both were legal. Both were commercially available. Both produced dependency. Neither was classified as especially dangerous, because the classification system that would later sort substances into legal and illegal had not yet been invented.
The missing classification was not a bureaucratic oversight. It was a structural condition that kept profits high and liability low. Patent medicine manufacturers profited from unregulated sale. Newspapers profited from patent medicine advertising. Railroads and wholesalers profited from moving the product. Pharmacists and general merchants profited from being the local outlet. Consumers received preparations that made them feel better in the short term and dependent in the long term. And because no institution had the authority to label the products as harmful, no institution bore the responsibility for the harm they caused. The dead infants were recorded as individual tragedies — sad, regrettable, but not systemic. Not yet.
The scale of what the patent medicine economy produced becomes visible only when you look at what was actually in the bottles.
Bayer’s Heroin, introduced in 1898, was marketed as a cough suppressant and a non-addictive alternative to morphine. The company’s advertisements appeared in medical journals and consumer publications. Bayer’s promotional literature described Heroin as safe for children. Physicians prescribed it for bronchitis, pneumonia, and tuberculosis. Bayer distributed free samples to physicians and hospitals across Europe and the United States.⁶ The word “Heroin” — capitalised, trademarked — appeared alongside aspirin in Bayer’s product catalogue. Both were new. Both were profitable. Both were legal. One of them would become the most prosecuted substance in American criminal history. In 1898, nobody reading those ads could have predicted which one.
Coca-Cola, formulated in 1886 by Atlanta pharmacist John Stith Pemberton, contained cocaine derived from coca leaves. The original formula used roughly 9 milligrams of cocaine per glass.⁷ Pemberton marketed it as a patent medicine — a “brain tonic” and cure for morphine addiction, which was itself a product of the patent medicine economy. Coca-Cola’s advertising pitched it as “delicious and refreshing,” a harmless pick-me-up for tired workers and respectable ladies. The cocaine was removed from the formula around 1903, not because of any law but because the company made a commercial calculation about changing public sentiment.⁸ The coca leaf extract remained, decocainised, and remains in the formula today.
Laudanum — a tincture of opium dissolved in alcohol — was among the most widely consumed medicines in America throughout the nineteenth century. You could buy it at the general store. Physicians prescribed it for everything from menstrual cramps to infant colic to “nervousness.” Working-class families used it as a painkiller because they couldn’t afford a doctor. Farm labourers dosed themselves to keep working through harvest. Women took it for conditions that men had decided were hysterical.⁹ The consumption was gendered and classed from the beginning: the bodies being managed were disproportionately female and disproportionately poor, and the management was chemical.
And then there were the infant preparations — an entire sub-industry of opiate-laced products designed for babies and young children. Mrs. Winslow’s Soothing Syrup was the most famous, but it had company: Godfrey’s Cordial, Atkinson and Barker’s Royal Infants’ Preservative, Dr. James’ Soothing Syrup Cordial, Street’s Infant Quietness. The names were reassuring. The contents were morphine, opium, or both, in doses calibrated to stop a baby from crying — which they did, because opiates suppress the central nervous system. Some babies stopped crying permanently. A British medical officer estimated in 1862 that opiate-based infant preparations were responsible for more infant deaths than scarlet fever and measles combined in industrial districts.¹⁰ The products continued to sell for another four decades.
These were not obscure products used by a marginal population. They were the American pharmacy. By the late 1890s, the United States was importing over 500,000 pounds of crude opium per year, the vast majority for domestic consumption in patent medicines and medical preparations.¹¹ Per capita opiate consumption in the United States was higher in the 1890s than at any point in the twentieth century — higher than during the heroin epidemic of the 1970s, higher than during the OxyContin crisis of the 2000s.¹² The difference was that nobody had a name for it. Dependency existed, massively and profitably, but the word “addiction” had not yet acquired its modern freight of moral condemnation and criminal classification. People who couldn’t stop taking laudanum were habituated, perhaps unfortunate, occasionally discussed in medical journals. They were not criminals. They were not “addicts” in the sense the twentieth century would construct. They were customers — and, from the industry’s point of view, excellent ones.
If you wanted to see what this looked like on the ground, you didn’t need a government report. You could walk into any small-town drugstore and watch the trade. Laudanum measured out by the ounce into a reused bottle. Paregoric sold “for the baby” with a wink. A bottle of bitters slipped across the counter to a man who couldn’t legally buy whiskey on Sunday. No paperwork. No labels beyond the brand name and a stream of promises. A national drug habit lived and moved through these ordinary transactions long before the state decided to call it a crisis.
The engine that kept this economy running — the mechanism that prevented information about harm from reaching the people being harmed — was not secrecy. It was advertising.
By the 1890s, patent medicine manufacturers were the single largest category of advertisers in American newspapers.¹² The revenue relationship was not incidental. It was structural. Newspapers depended on patent medicine advertising for between one-quarter and one-third of their total advertising revenue.¹³ This created a dependency of its own: the newspaper depended on the manufacturer, the manufacturer depended on the newspaper, and neither had an incentive to publish information that would damage the other.
The result was a media environment in which the most widely consumed drugs in the country were also the most heavily promoted, and the outlets doing the promoting were the same outlets that might otherwise have reported on the harms. When physicians published warnings about patent medicine contents in medical journals, those warnings rarely crossed into the popular press. When coroners recorded infant deaths from morphine-laced syrups, the inquests were local news at best. The system was not hidden. It was simply profitable enough that nobody with a platform had a financial reason to expose it.
Some newspapers went further than silence. They signed contracts. The “red clause” — named for the colour of ink in which it was printed — was a standard provision in patent medicine advertising agreements that voided the advertising contract if the state in which the newspaper operated passed any law restricting patent medicine sales.¹⁴ The clause turned every newspaper that signed it into an active lobbying force against drug regulation. Editors who depended on patent medicine revenue were not merely failing to report harms. They were contractually obligated to fight legislation that would protect their readers from those harms. The economic structure of American journalism in the 1890s made the press an arm of the patent medicine industry — not through envelopes of cash under the table, but through the ordinary operation of advertising markets.
For a small-town editor whose sheet might go under without that money, the red clause was a gun on the table. Run our ads, keep quiet about regulation, or watch your main revenue stream vanish the moment a legislator proposes a labelling law. Multiply that calculation across hundreds of towns and you get a national information blackout enforced not by censors, but by contracts and balance sheets.
This arrangement — media revenue dependent on drug company advertising, producing a structural inability to report on drug company harms — was not unique to the 1890s. Arthur Sackler, the advertising pioneer who would later build the marketing strategy for Valium and lay the groundwork for OxyContin’s promotional architecture, made his career by understanding exactly this mechanism. Sackler’s innovation in the 1960s was to redirect pharmaceutical advertising into medical journals, making the journals dependent on pharma revenue in the same way newspapers had been dependent on patent medicine revenue seventy years earlier.¹⁵ The scale changed. The channel changed. The mechanism — media capture through advertising dependency — was identical. What the patent medicine economy invented, the pharmaceutical industry perfected.
The few journalists who did expose the industry operated against the financial interests of their own employers. Samuel Hopkins Adams’ “Great American Fraud” series in Collier’s Weekly in 1905 and 1906 was a landmark — Adams documented the contents of patent medicines, named the manufacturers, and exposed the harm.¹⁶ He published tables of ingredients. He reprinted labels. He made it impossible for anyone who read the series to pretend they didn’t know what Mrs. Winslow’s Soothing Syrup and its cousins contained. But Adams could publish the series in Collier’s precisely because Collier’s had made a corporate decision to refuse patent medicine advertising, which most newspapers had not. The structural constraint was real. Exposure required independence from the revenue stream, and most outlets didn’t have it.
The bodies at the centre of this economy were not abstractions. They were infants dosed for teething pain. They were women taking laudanum for menstrual cramps because the medical profession treated female pain as hysteria and the pharmacy counter offered the only relief that didn’t require a physician’s condescension. They were workers — miners, farmhands, factory labourers — managing pain from injuries sustained in workplaces that offered no compensation, no disability coverage, no alternative to self-medication. They were Civil War veterans, whose morphine dependency had been produced by the state itself and then reframed as individual weakness.
The gendered dimension was sharp and early. Surveys conducted by physicians and pharmacists in the late nineteenth century consistently found that women constituted a majority — in some studies, two-thirds — of habitual opiate users.¹⁷ The pattern was not pharmacological but structural. Women were prescribed opiates for a range of conditions that reflected medicine’s inability or unwillingness to address their actual health needs: “female complaints,” “nerves,” “domestic anxiety.” The prescriptions produced dependency. The dependency was then cited as evidence of female constitutional weakness. The system created the condition and blamed the patient — a mechanism that would repeat, with different populations and different substances, across every stage of American drug history.
The labour dimension was just as clear. Working-class Americans consumed opiates at rates that reflected the conditions of their labour. An 1885 survey of Iowa pharmacies found that habitual opiate purchasers were disproportionately labourers and their wives, purchasing laudanum and paregoric to manage pain, fatigue, and the grinding conditions of agricultural and industrial work.¹⁸ In factory towns, pharmacists knew their regular customers — the mill worker who came in every Saturday for a bottle of laudanum, the miner’s wife who bought paregoric by the half-pint. The dependency was visible at the counter and invisible in the statistics, because no institution was counting. This was chemical management of the workforce — the same function that amphetamines would serve for soldiers and factory workers in the 1940s, that tranquillisers would serve for housewives in the 1960s, that OxyContin would serve for injured workers in the 2000s. The substance changes. The function — managing the body for continued productivity in conditions that damage it — persists across every stage of the system this book traces.
You can also see, in embryo, the pattern that will later define the American overdose crisis: drugs used to patch over injuries produced by work that is too hard, too long, and too poorly paid; no structural relief; a bottle as the only available fix. When those bottles are sold over the counter, the worker is a “customer.” When the same chemistry moves to a different channel a century later, the worker becomes a “drug offender.” Nothing fundamental about the body changes. What changes is the way the state chooses to name what is happening to it.
What did not yet exist was a racial classification mechanism. That was coming. By the 1870s and 1880s, anti-Chinese sentiment on the West Coast was producing the first racialised drug legislation in American history: San Francisco’s opium den ordinance of 1875, which criminalised the smoking of opium in the specific locations where Chinese immigrants consumed it while leaving the same substance legal in every other form.¹⁹ The ordinance had nothing to do with public health and everything to do with labour competition — Chinese workers were being driven out of industries where they competed with white labour, and drug legislation was one of the tools. But this machinery was still local and fragmented. The national racial classification of drugs — the system Harry Anslinger would build into federal policy — was still decades away.
By the turn of the twentieth century, the patent medicine economy had produced a set of conditions that could not be sustained — not because the public demanded change, but because specific institutional interests needed a boundary that did not yet exist.
The American Medical Association, reorganised and professionalised in the 1890s and 1900s, needed the authority to determine what counted as medicine and what didn’t.²⁰ As long as anyone could sell anything as a cure, the physician’s professional authority was undermined. Classification — the legal distinction between approved medicine and quackery — was the AMA’s route to professional monopoly. The motive was not purely public health. It was institutional power.
Harvey Wiley, chief chemist at the U.S. Department of Agriculture and the architect of what would become the Pure Food and Drug Act of 1906, waged a decade-long campaign to require labelling of patent medicine ingredients.²¹ Wiley’s “poison squad” experiments, in which volunteer subjects consumed preservatives under controlled conditions, were public theatre as well as science. He took his case to women’s clubs, farmers’ organisations, and reformers who had watched relatives die after taking “safe” remedies. His fight was real and consequential — the 1906 Act was the first federal legislation to require truthful labelling and the first to establish federal authority over drug products. But the Act did not prohibit anything. It required labels. The patent medicine manufacturers who survived — and most did — simply reformulated, relabelled, and continued selling. The market adapted. The bodies remained.
On the other side of Wiley’s campaign stood the Proprietary Association of America, the trade group for patent medicine makers. Its members coordinated legal strategy, drafted model editorials for friendly newspapers, and denounced regulation as an attack on “freedom” and “choice.” They warned that any attempt to put ingredients on labels would “alarm” the public and damage honest business. They were right about the first part: full disclosure would have alarmed anyone who realised they were feeding their child a narcotic. That was exactly why they fought it.
The Pure Food and Drug Act created the infrastructure for federal regulation. It established the principle that the government had authority over what went into consumer products. It created the bureaucratic ancestor of the FDA. And it created the conditions under which a more aggressive boundary — not labelling but prohibition, not disclosure but criminalisation — could be drawn. That boundary would arrive in 1914, with the Harrison Narcotics Tax Act, and it would transform the entire structure of the American drug economy overnight.
But in 1906, none of that had happened yet. What existed was a market. The market sold products containing opium, morphine, heroin, cocaine, and cannabis to millions of Americans without restriction, without disclosure, and without criminal penalty. The market produced dependency on an industrial scale. The market killed infants, managed women, medicated workers, and generated enormous profits for manufacturers and the newspapers that advertised their products. Everything that the twentieth century would call “the drug problem” already existed in the nineteenth century — except the classification. The drugs were there. The dependency was there. The profit extraction was there. The bodies were there. What wasn’t there was the boundary.
The boundary had to be built. And the people who built it were not humanitarians. They were physicians consolidating professional authority, bureaucrats expanding federal power, moralists weaponising racial anxiety, and politicians discovering that drug classification was one of the most effective tools of population management ever devised. The boundary would not stop dependency. It would sort it — legal on one side, criminal on the other — and every institution that drew the line would profit from both sides.
That sorting is the subject of the next four chapters. But its precondition — the proof that the system operates without any boundary at all, that dependency is a product of markets and not of molecules — is here, in the patent medicine economy, in the dead infants, in the unlabelled bottles, in the advertisements that newspapers couldn’t afford to refuse.
Mrs. Winslow’s Soothing Syrup was legal the day it killed a baby in Salford. Every institution that would later claim to protect the public from dangerous drugs did not yet exist. The morphine in the bottle was the same morphine that would fill prison cells a century later. The only difference was the label — and in 1884, there was no label at all.